ALAN at EHA 2026
Some words from Charles, ALAN Steering Committee Member
My third EHA Congress was a fascinating experience, giving me the perfect opportunity to continue my journey in patient advocacy. There was no doubting that patient voice formed an integral part of this year’s event, with many clinical sessions incorporating patient preferences and quality of life in a way that just wasn’t the case two years ago during my first Congress.
Congress was a great opportunity to progress my work with EHA’s AYA Taskforce, which has just ‘evolved’ into a Specialised Working Group (SWG). Its new status gives it even more weight within the structures of EHA, and I’m pleased to be taking a role on its Steering Committee going forwards. During our session, the Taskforce reminded itself of our recently published AYA Strategy with its four goals of Analysis, Improving Standards of Care, Policy, Education, and Research, which will be implemented over the coming years. Our efforts will be boosted by the fact the AYA will be EHA’s Topic in Focus (TiF) for the next four years, granting us more capacity and resources to bring better AYA care to life across Europe.
During Congress, I and other young patient advocates met with members of the Patient Advocacy Committee (PAC), where we identified key blockers in terms of resourcing and structure. I’m looking forward to working with the PAC to overcome these challenges and ensure it remains as effective as it can be in influencing the presence of patients at EHA Congresses and beyond.
It was a delight to see the Acute Leukaemia Advocates Network presenting two posters during Congress this year, in collaboration with CML Advocates, CLLAN, HM-Pro, and QOL-One. These posters explored different approaches to measuring patient quality of life, including by proxy assessments of caregivers and the physical and psychosocial impact on them during a patient’s diagnosis, treatment, and follow up. This poster specifically raised some interesting questions about how patient reported outcome measures (PROMs) should be used in clinical trials in future!
The next 12 months will be an exciting time for AYA patient advocacy, with the aim being to present our own poster at Congress 2027 on the results of our AYA sexual health survey. A webinar is also in the works for Q3 2026, so stay tuned!

Key Insights from ALAN’s Presentations at EHA2026
This year’s European Hematology Association Congress in Stockholm was a milestone moment for patient advocacy in hematology. The Acute Leukemia Advocates Network (ALAN) was proud to contribute research, presentations, and a persistent call to action: that patient experience data must move from the margins to the centre of how we develop, evaluate, and approve medicines for people with acute leukemia.
Across multiple sessions and poster presentations, ALAN’s work this year made one thing abundantly clear: survival statistics do not tell the full story. Here is what we shared — and why it matters.
Why Patient Experience Data Must Shape Drug Approval
In the opening, we set the scene with a central challenge: regulatory bodies including the FDA and EMA increasingly value patient input — yet in practice, patient perspectives arrive late, remain anecdotal, and often fail to capture what patients actually experience in daily life.
ALAN’s patient experience data — drawn from over 2,500 leukemia patients across more than 80 countries — demonstrated several critical findings:
- Patients with acute leukemia largely prioritise treatment efficacy, but quality of life and convenience also matter — and these priorities shift across the treatment journey.
- Patient priorities differ meaningfully from general population preferences, which has direct implications for how economic evaluations and HTA assessments are conducted.
- Cognition and tiredness emerge as critical domains that are nearly absent from standard EQ-5D evaluations — yet patients rank them on a par with pain and discomfort.
- Caregiver burden is substantial and systematically overlooked in benefit–risk assessments.
The key message: if we do not systematically collect what matters to patients, we risk approving medicines that prolong life — but ignore how that life is lived.
PROMs and FROMs: The Key to Patient and Family-Centred Care
A full presentation made the case for embedding Patient-Reported Outcome Measures (PROMs) and Family-Reported Outcome Measures (FROMs) as standard clinical practice — not merely research tools. ALAN’s evidence base, spanning studies from 2019 to 2026, shows consistently that what clinical trials measure and what patients experience are frequently misaligned.
What trials measure vs. what is often missing:
| What Trials Measure | What is Often Missing |
| Complete remission rate | Fatigue & cognitive impact |
| Overall survival | Emotional distress / depression |
| Progression-free survival | Social isolation & relationships |
| Adverse event grading (CTCAE) | Caregiver burden & family QoL |
| Eating habits & daily function |
The call to action is clear — and urgent. ALAN calls for:
- Immediate: All hematology centres to adopt validated PROMs and FROMs at diagnosis, during treatment, post-treatment, and at relapse — alongside family FROMs.
- Short-term: Quality of life to become a co-primary endpoint in all new acute leukemia clinical trials, with shared validated instruments and genuine patient involvement in trial design.
- Medium-term: Real-world registries linking trial PRO/FRO data to clinical outcomes; targeted psychosocial, financial, and practical support services commissioned from this evidence.
- Long-term: Integration of PROMs and FROMs into EU Joint Clinical Assessments and national HTA frameworks.
Beyond the Blood Count: Qualitative Research and the Invisible Carer
The final presentation drew on ALAN’s multinational qualitative study of 60 informal carers across the UK, US, France, Germany, Italy, and Spain. Semi-structured interviews, analysed using reflexive thematic analysis, generated three interlinking themes:
Impact of the Carer–Patient Dynamic
Relationships deepen under adversity but also fracture under the weight of role conflict. Partners become nurses; parents become patients. Some relationships come close to breaking point.
Balancing Multiple Roles
47% of carers in the study were working full-time while providing intensive caregiving. Financial toxicity — lost income, insurance costs, depleted savings — was a near-universal experience.
Putting the Patient First
Carers rapidly become lay experts in leukemia while consistently deprioritising their own health, social life, and wellbeing. Treatment preference discordance is common: carers tend to prioritise quality of life for the patient, while patients often prioritise survival.
Key statistic: 58% of informal caregivers reported a very large or extremely large impact of illness on their own quality of life. 15% reported no support network whatsoever.
The message to clinicians was direct: the carers you never see are in every room with every patient. Qualitative research makes them visible — and what be comes visible can be acted upon.
Family Carer Burden and Proxy PRO Concordance (PF1399)
This poster examined whether family carers can serve as reliable proxies for patient-reported outcomes — a critical question for trial design and clinical practice. The findings revealed an important nuance:
- Over 25% of carers provided more than 36 hours of care per week — a level of intensity comparable to full-time employment.
- Carers showed moderate agreement with patients on observable domains such as physical functioning and symptoms.
- However, carers consistently underestimated emotional wellbeing and overall QoL — particularly in acute leukemia.
- Agreement was weakest for emotional behaviour (kappa = 0.17 in acute leukemia; p = 0.04), confirming that carers cannot substitute for direct patient reporting on psychosocial domains.
- Integrating both patient and carer assessments provides a more complete picture for holistic leukemia management.
Conclusion: Carer input is valuable but should complement — not replace — direct patient-reported outcomes.

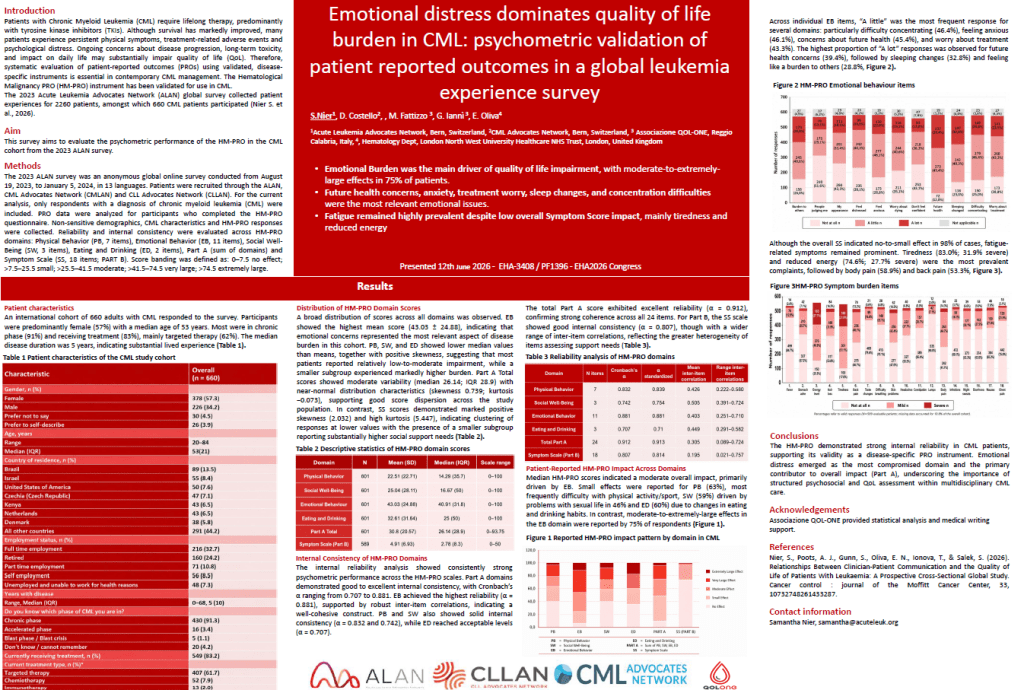
Emotional Distress Dominates Quality of Life in CML (PF1396)
A poster presenting psychometric validation of the HM-PRO instrument in 660 CML patients confirmed that emotional burden — not physical symptoms — is the primary driver of quality of life impairment in this population.
Key findings:
- Moderate-to-extremely-large effects in the emotional behaviour domain were reported by 75% of respondents.
- Future health concerns (39.4%), sleeping changes (32.8%), and feeling like a burden to others (28.8%) were the most frequently reported severe emotional issues.
- Despite a low overall symptom score, fatigue-related symptoms remained prominent: tiredness (83%) and reduced energy (74.6%) were near-universal.
- The HM-PRO demonstrated excellent internal consistency (Cronbach’s α = 0.912 for Part A), confirming its validity as a disease-specific PRO instrument for CML.
Conclusion: Structured psychosocial and QoL assessment using validated, disease-specific instruments must become standard in multidisciplinary CML care.
Sleep Disturbances: A Clinically Meaningful Unmet Need (PF1394)
A new poster presented data from an international cohort of 329 patients with hematological malignancies, examining sleep disturbances after diagnosis. The findings were striking:
- 80% of respondents who completed the Pittsburgh Sleep Quality Index (PSQI) reported poor global sleep quality.
- 59.3% reported their sleep had become worse following diagnosis.
- Anxiety, fatigue, night sweats, and pain were the main sleep-disrupting symptoms.
- A profound communication gap was identified: most patients had never discussed their sleep with their healthcare team, and 32.5% rated clinical management of their sleep negatively.
- CML patients exhibited significantly higher sleep disruption burden than MDS patients across multiple PSQI domains.
- Non-pharmacological strategies were preferred by patients, yet educational resources on sleep management remain largely unavailable.
Conclusion: Sleep should be recognised as a clinically relevant quality-of-life domain and a formal target for supportive care in hematology.

In Conclusion
EHA2026 reinforced what ALAN has been saying for years: the evidence base for patient-centred care in hematology is no longer a ‘nice to have’. It is robust, it is global, and it demands action.
Ultimately, PED, PROMs, FROMs, and qualitative research ensure that new medicines are not only clinically effective — but meaningful to the people living with the disease, and the people who love them.
The time for pilot projects and ‘we should’ is over. We need to act now.